What are we collecting?
Overview
NADAbase incorporates the Alcohol and Other Drug Treatment Services National and NSW Minimum Data Set data and the Client Outcomes Measures.
Minimum Data Set
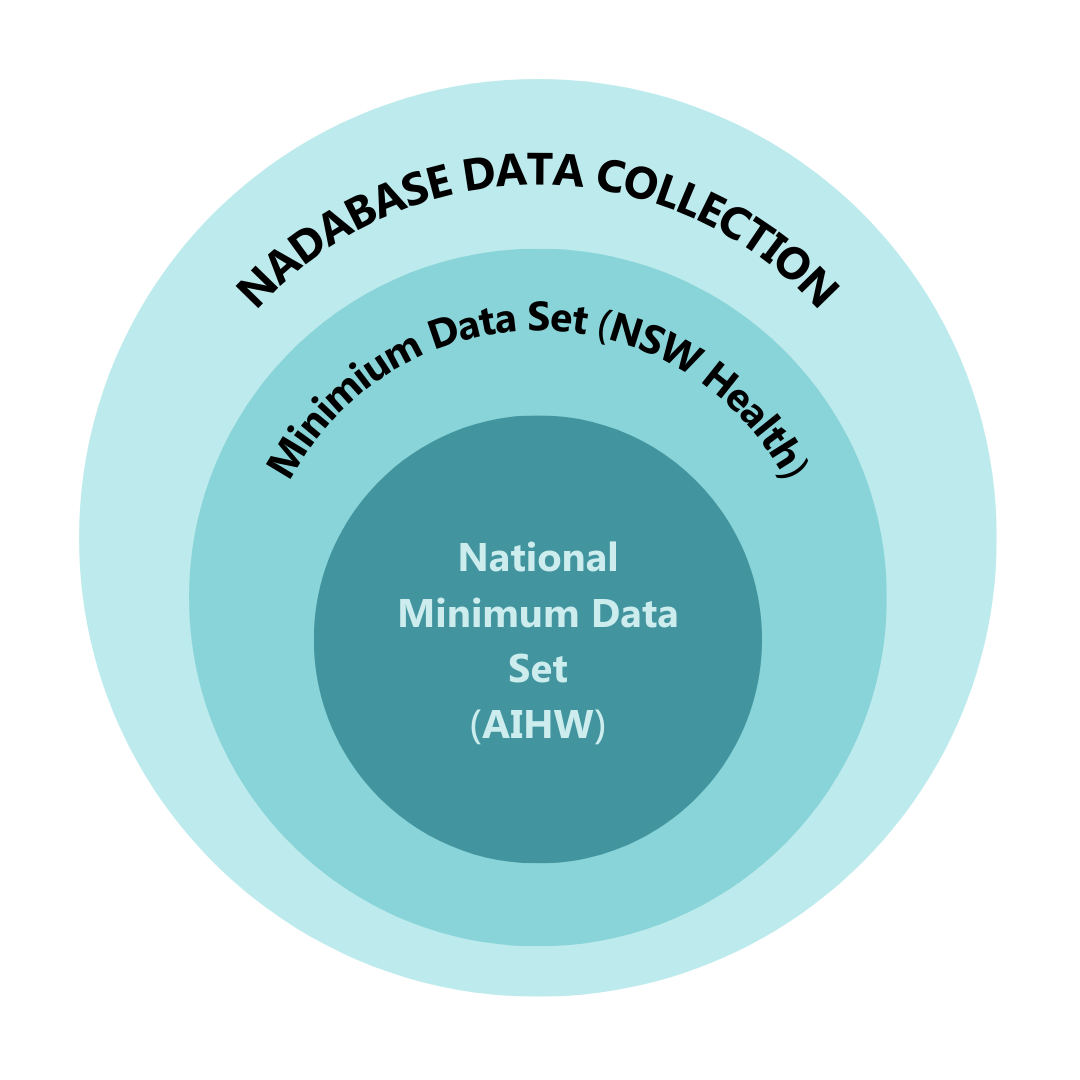
AOD treatment providers funded by NSW Health and/or PHNs are obligated to collect data for every client they assist. The specific data required depends on the funding contract. To streamline this process and ensure completeness, NADAbase follows the NSW Minimum Data Set (MDS), which contains a comprehensive amount of data. This set of data overlaps with the National Minimum Data Set requirements.
While the National MDS consists of 33 items, the NSW MDS consists of 44 items. Due to the diverse funding received by NADA members, NADA has opted to adopt the NSW MDS to guarantee the collection of all necessary data items from both sets.
Client Outcome Measures
NADAbase gathers Client Outcome Measures (COMS). Collecting data on client outcomes can inform individual treatment approaches and provide valuable insights for organizations and the entire sector. This enhances reporting accuracy and facilitates advocacy for adequate resources. Read more about the Importance of COMS [PDF]
The COMS aims to be comprehensive enough to cover a wide range of client outcomes resulting from treatment, while also being concise to avoid imposing excessive data collection burdens. Moreover, the COMS must be applicable across various service types and program categories, such as residential facilities, counseling, and case management programs.
The following four outcome domains form the COMS:
- Drug and Alcohol Use: The Severity of Dependence Scale (SDS) is a brief screening measure of psychological aspects of dependence. This short yet effective tool is easy to administer to evaluate the level of severity of substance dependence perceived by the client.
- Psychological Health: The Kessler 10+ scale (K10+) is a widely used, simple self-report measure of psychological distress, which can be used to identify those in need of further assessment for anxiety and depression. It is based on questions about the individual’s level of nervousness agitation, psychological fatigue and depression in the past 4 weeks.
- Health and Social Functioning: The World Health Organisation Quality of Life 8 questions (WHO QoL-8) was designed for use as a very short and concise quality of life instrument. It has been used and validated across a range of populations, including in drug and alcohol settings and with those with mental health disorders. It has been validated cross culturally and in the Australian context. It has been found to be reliable and valid in both older and younger people and has been extensively tested in both psychiatric and drug and alcohol contexts.
- Blood Borne Virus Risk: 4 items on injecting drug use and overdose from the BTOM-C
Why should we collect outcome measures if they’re not required?
In recent years, NSW Health and PHNs have begun to integrate the collection of client outcome measures into certain funding contracts, although it’s not yet a mandatory part of all data collection processes.
The purpose of monitoring outcomes is to determine if a person’s treatment experience leads to positive changes and improvement. It’s important to note that while outcomes monitoring doesn’t directly prove that treatment caused these changes, it does help showcase the effectiveness of treatment from the client’s perspective.